All 6 CMS timepoints
SOC, ROC, FUP, RFA, TRN, DC, DAH. Timepoint controls section visibility automatically — you don't see Discharge questions on a Start of Care.
Clinical & EHR
Clinical software your DON can hand to a brand-new field nurse without a five-day training class. Schema-driven forms, auto-save every 2.5 seconds, sticky section nav, and a single workflow: Draft → Validate & Complete → Sign → QA Review → Locked.
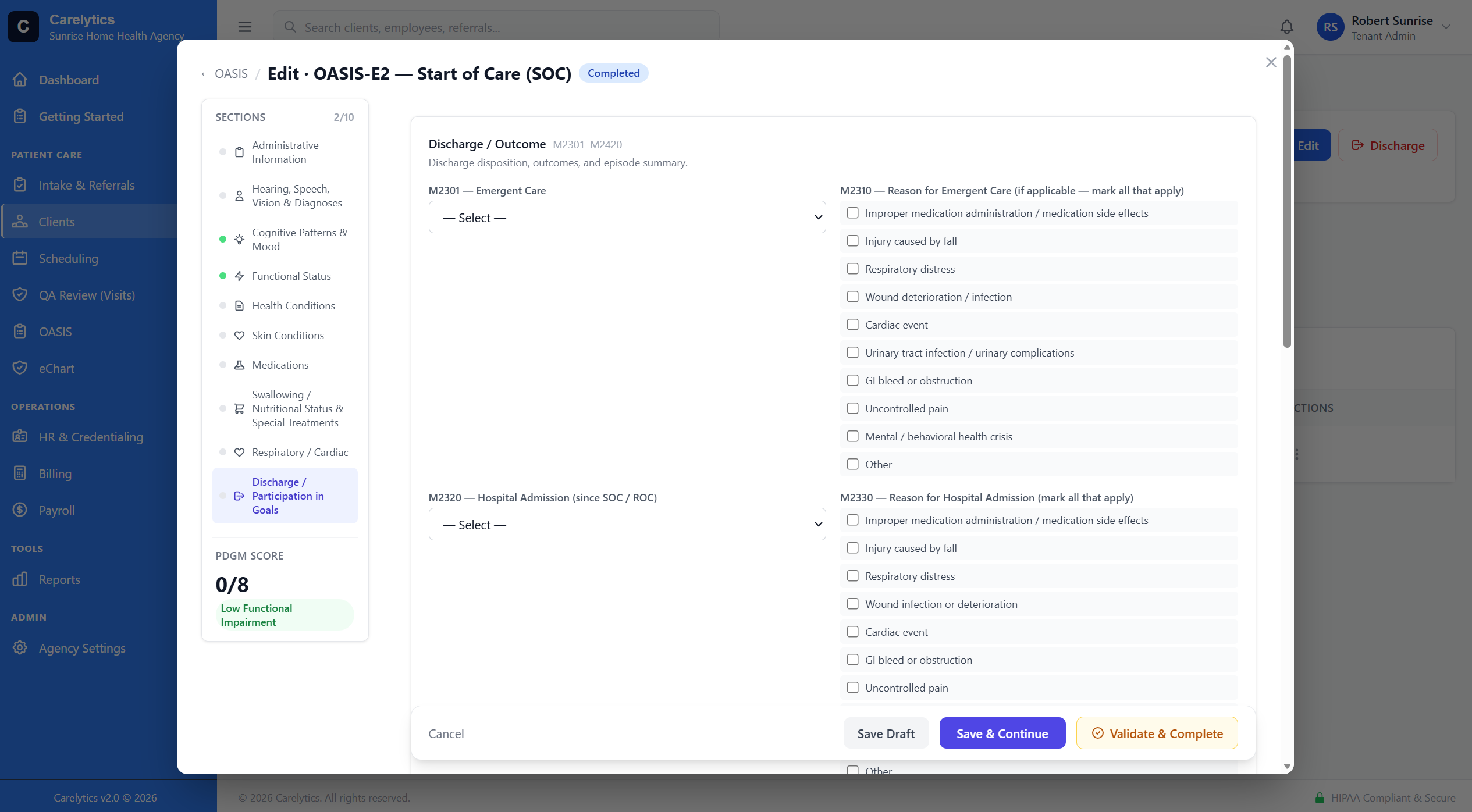
OASIS-E2
Status transitions are button-driven. No "is this draft or in-progress?" guessing. Every transition is audit-logged with user, IP, and timestamp.
SOC, ROC, FUP, RFA, TRN, DC, DAH. Timepoint controls section visibility automatically — you don't see Discharge questions on a Start of Care.
Sections A through Q. M0010–M2401 plus all OASIS-E2 additions: BIMS, PHQ-9, CAM, Health Literacy, Social Isolation, GG self-care/mobility.
System admins can force-complete an OASIS with errors when clinically justified. Reason required, signed, surfaced as an orange override banner for everyone who opens the OASIS afterward.
OASIS Inactivation
Wrong patient on a signed OASIS. Wrong timepoint. Wrong SOC date. Duplicate. Event that
didn't actually happen. The CMS fix is the iQIES inactivation — CORRECTION_NUM = XX —
and it's non-negotiable: a bad OASIS sits in iQIES corrupting your HHRG, HHVBP, and Care
Compare metrics until you formally void it. The next PDGM claim that references the bad
record fails with reason code 38107.
Clinical Manager or Admin clicks Inactivate on a locked OASIS, confirms a 20+ character reason, and Carelytic snapshots the original key fields (M0010, M0014, M0016, M0020, M0030, M0040, M0066, M0090, M0100). Next iQIES export emits CORRECTION_NUM=XX referencing the snapshotted tuple — iQIES finds the original record and voids it cleanly.
If the event actually happened (and just had a key-field error), the inactivation banner offers Create Replacement Assessment — clones every section's data into a fresh draft so the clinician corrects the wrong field and re-signs. The new submission is a brand-new original (CORRECTION_NUM=00), not a modification.
CMS rejects inactivations more than 24 months from M0090. Carelytic enforces that pre-flight so you don't roundtrip a fatal iQIES error. Every inactivation is audit-logged with user, IP, reason, before/after snapshot, and a list of overlapping claims flagged for repricing.
The clinical.inactivate_oasis permission ships off by default for everyone except
Agency Admin and Clinical Manager — inactivation has billing and quality-measure consequences and
is a State-survey-reportable event. We ship the right defaults so you don't have to remember to set them.
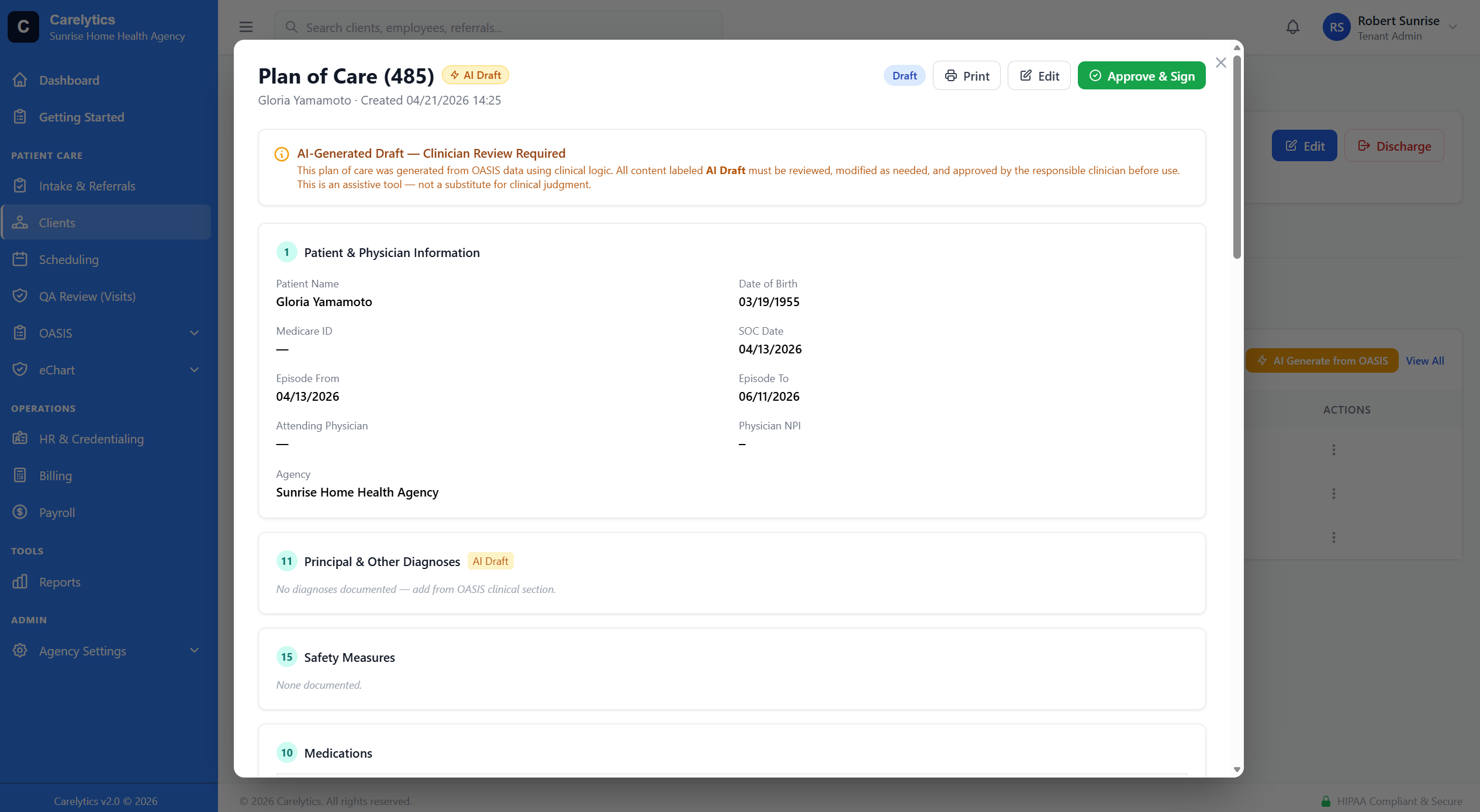
Plan of Care
The minute a clinician signs OASIS and QA approves, the 485 is ready. Medications, diagnoses, DME, safety, prognosis, goals, and interventions all auto-populate from OASIS data and the patient's current chart state.
Multi-discipline charts
17-section visit note canonical pattern. AI SOAP draft, Pre-Sign QA, Carry-Forward.
Evaluations and visit notes with discipline-specific assessments and goals.
Psychosocial evaluation with SDOH, support system, financial barriers.
Aide care plan + visit note. Supervisory visit form for RN sign-off.
Hourly PDN daily note. Auto-populated from client profile, OASIS, payer, episode.
Standalone-allowed (clinicians can document an emergency without a scheduled visit).
Active list, allergies, reconciliation, MD notification on changes.
Per-dose administration tracking with timestamps, refusals, and PRN documentation. Tied to the active medication list — no double entry.
Build agency-specific forms without code. Schema-driven renderer.
Triggered clinical assessments
OASIS items don't live alone — M1306 implies a wound assessment, J1900 implies a fall-risk re-eval, C0500 ≤ 7 plus pain implies PAINAD. Most platforms leave it to the clinician to remember. Carelytic's trigger framework reads the OASIS as it's being completed and creates the matching assessment stubs automatically — quietly, never as pop-up alerts.
All scored, banded, and persisted. Score auto-calculation lives in the model — never trust client-submitted totals.
The framework follows AHRQ guidance: passive sidebar checklists outperform interruptive alerts on completion AND clinician satisfaction. Every trigger fits one of three tiers:
M1306 (pressure injury) auto-creates a Wound stub per ulcer counted in M1311. J1800/J1900 auto-creates STEADI. C0500 = 99 (uninterviewable) auto-creates Mini-Cog. M2102 ADL assistance + dementia auto-creates MCSI. Living alone (M1100) + ADL deficit auto-creates Lawton plus a soc-work task.
New wound noted on the SN note auto-creates Wound + Braden re-eval. Fall reported with injury triggers a safety-floor STEADI. Cognitive change auto-creates Mini-Cog. Caregiver-strain checkbox auto-creates MCSI. Weight loss ≥ 5% baseline triggers Braden + nutrition flag.
The OIG's home-health audit reports cite missing wound assessment + missing STEADI on injury falls as top failure points. Carelytic blocks OASIS sign on those exact items unless the matching assessment is completed or formally dismissed with a reason — both audit-logged.
The framework is dev-authored. When CMS adds an OASIS item or your QA team identifies a new gap, registering a trigger is roughly 30 lines of Python — not a vendor change-request.
Carelytic surfaces a current hospitalization-risk score on every patient — drawn from whichever data is most recent (OASIS M1033 or a standalone risk assessment for agencies that don't run OASIS). The 0–9 score and risk band show on the client header, the visit detail modal, and the Clinicals dashboard so caregivers and the office see the same number.
An upward score transition (e.g. moderate → very-high) auto-creates a ClientAlert with severity matched to the new band — quiet on downward moves, never noisy. A nightly Celery sweep flags any client whose risk assessment is > 60 days stale for re-evaluation.
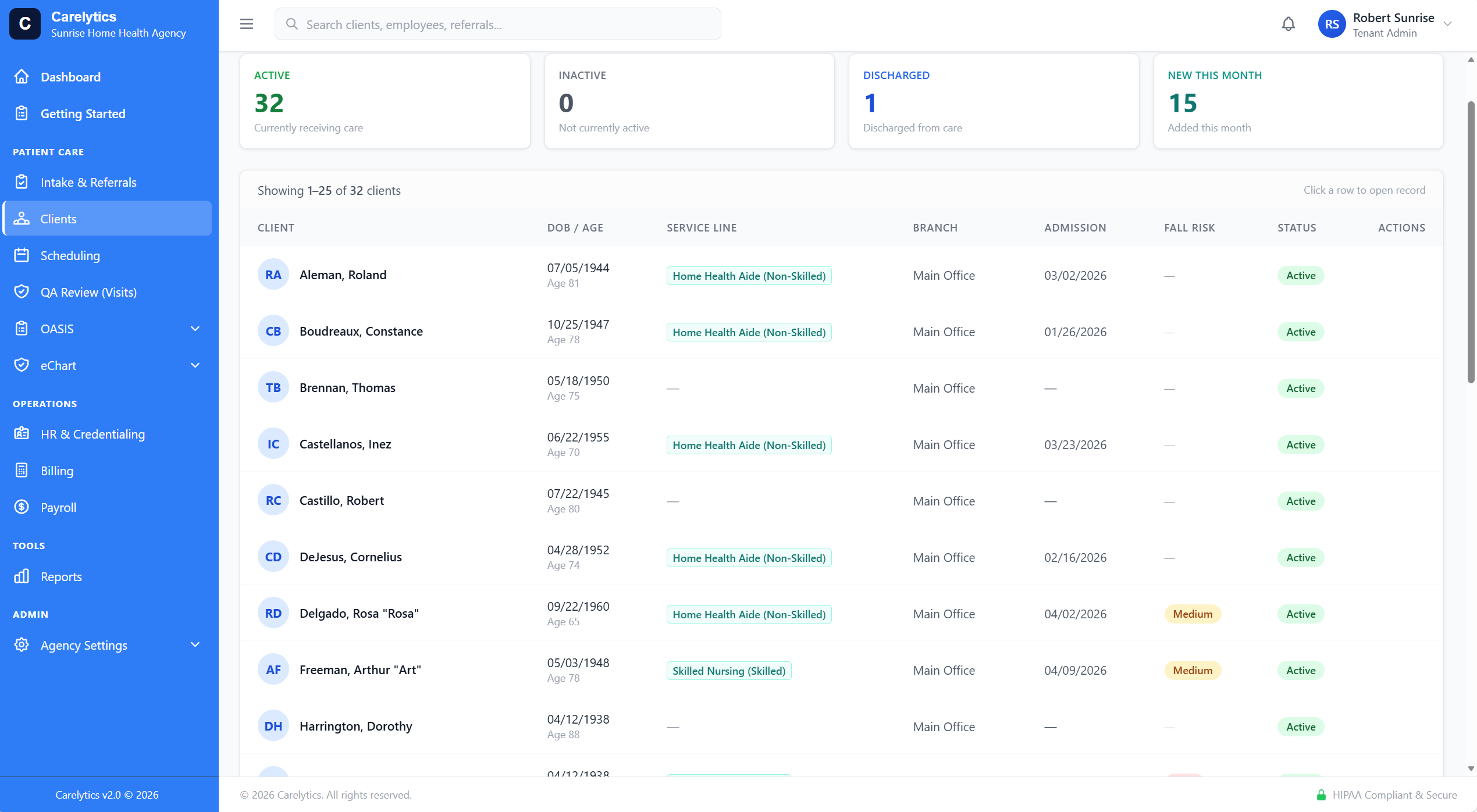
Scheduler → Chart
No more "I documented but forgot to clock in." Every visit on the calendar carries an eChart type. The clinician hits Start Documentation, the platform routes to the right form with patient, scheduled times, and clinician already filled in. The visit and the chart stay linked forever — for billing, for QA, for audit.
Lock-on-sign
Action bar grays out. Form inputs become read-only. Delete blocked. Backdoor /edit URLs return 403. There's no version of "open the locked form, change a field, hope no one notices."
User, IP, timestamp, and field-level diff for every status change and CRUD operation — including login/logout. Queryable per entity from the activity log.
Signed forms enter the QA queue. Reviewer can Approve (→ locked) or Return with reason (→ clinician edits → re-validate). All routed by RBAC; only the QA role sees the queue.
Physician orders & medications
Physician orders aren't generic — a wound-care order has different fields than a respiratory therapy order than a DME order than a physical therapy frequency change. Carelytic ships 14 order types with type-specific fields, smart defaults, and one-click links to the patient and the clinician.
Each surfaces only the fields that actually matter for that order shape:
Physicians still fax medication lists as PDFs. Most platforms make you re-key each line item. Carelytic's AI scanner reads the inbound fax (or any uploaded PDF), extracts every medication line, and proposes structured records with name, dose, route, frequency, indication, and start date.
The clinician reviews and accepts each line — no auto-apply. Every accepted suggestion cites the chart text it came from. Fits the same OIG-safe AI standard as the rest of the platform: improve documentation accuracy by anchoring to evidence, never optimize for billing.
Click an order row → read-only detail modal. Edit button inside opens the type-locked form (so a wound order doesn't morph into a med change after the fact). Delete prompts a styled confirmation modal — no native browser confirm() dialogs anywhere in the platform.
Once a physician signs an order, the form is read-only. Editing requires creating an addendum — the original signed order is immutable. Same audit standard as OASIS and SN notes.
Physician profile carries phone, fax, NPI. Order forms pre-populate the contact info so clinicians don't re-enter it on every order. Physician-fax outbound goes straight to the integrated fax line for auto-tracked delivery.
Visual Form Builder
Every clinical form in Carelytics — including OASIS — uses the same JSON schema renderer. Agency-specific forms (compliance audits, new-hire orientation, peds variants) ship the same way system forms do — configured in the UI, not in code.
16 field types — drag, drop, save
Red / amber / blue / teal / purple section headers with icon badges. Visual hierarchy across long forms.
Body-system sections get an "All Normal" button so a routine assessment is one click instead of twelve.
Agency admins review every form exactly as a clinician would see it — submit and sign actions disabled. No risk of altering data while reviewing.